


ABSTRACT
Background and Aim: Rabies remains one of the most lethal zoonotic diseases worldwide, causing substantial public health and economic burdens, particularly in low- and middle-income countries. Effective rabies control requires integrated surveillance systems that capture both animal and human health events within a One Health framework. The Emergency Prevention System for Animal Health (EMPRES-i Plus) is a global event-based surveillance platform that compiles rabies reports from multiple official sources. This study aimed to describe global spatiotemporal patterns of confirmed rabies reports recorded in EMPRES-i Plus between 2014 and 2024 and to evaluate their relevance within a One Health surveillance context.
Materials and Methods: A retrospective descriptive surveillance study was conducted using confirmed rabies records retrieved from the EMPRES-i Plus Global Animal Disease Information System. Data covering the period from January 1, 2014, to December 31, 2024, were extracted and cleaned before analysis. Reports were categorized according to geographic region, host type, and source of confirmation. Animal entries were analyzed at the report level, whereas human records were evaluated on an individual case basis. Descriptive statistics were used to summarize temporal trends, regional distributions, host categories, and geographic patterns.
Results: A total of 1,510 confirmed rabies reports were identified across Africa, the Americas, Asia, and Europe. Asia contributed the highest number of reports (n = 1,056), followed by the Americas (n = 319), Europe (n = 91), and Africa (n = 44). Annual reporting fluctuated considerably, with the highest number recorded in 2014 (n = 302). Most reports (74%) originated from the World Organization for Animal Health reporting system. Domestic animals accounted for the majority of reports (n = 1,326), whereas wild animals accounted for 176 reports and captive animals for only 2 reports. Human rabies cases were limited within the database, with 27 reported cases and 20 associated deaths, all occurring in Africa and Asia. Spatial visualization revealed a widespread geographic distribution of reported rabies events, although reporting intensity varied across regions.
Conclusion: Global rabies reporting within EMPRES-i Plus demonstrates marked regional and host-category variation, with domestic animals representing the principal reported reservoir and Asia contributing most reports. The findings emphasize the importance of strengthening harmonized One Health surveillance systems, improving cross-sectoral data integration, and enhancing reporting consistency to support progress toward global rabies elimination goals.
Keywords: animal–human interface, EMPRES-i Plus, event-based surveillance, global surveillance, One Health, rabies, spatiotemporal analysis, zoonotic disease surveillance.
INTRODUCTION
Rabies is a fatal viral zoonotic disease caused by Lyssavirus, a ribonucleic acid virus belonging to the family Rhabdoviridae [1]. Rabies is primarily transmitted through the bites of infected dogs and other mammals, including cats, foxes, and bats. The principal reservoir and transmission hosts vary geographically. In the Americas and Europe, wildlife species such as red foxes and bats constitute important reservoirs, whereas domestic animals remain the predominant source of transmission in many parts of Asia and Africa. Brazil has recently reported an increase in feline rabies cases, resulting in the loss of its 28-year rabies-free status [2, 3]. Clinically, rabies occurs in two major forms. Furious rabies is characterized by hyperactivity, hallucinations, hydrophobia, and impaired coordination, whereas paralytic rabies is associated with progressive muscle paralysis and the gradual development of coma [4]. Owing to its severe neurological manifestations, rabies remains almost universally fatal once clinical signs appear, with death typically occurring within days to weeks after symptom onset [4].
Estimates of the global rabies burden vary considerably. The Global Burden of Disease (GBD) study estimated approximately 10,000 rabies-related deaths in 2021, whereas Hampson et al. [6] reported that rabies causes approximately 59,000 human deaths annually worldwide [5, 6]. Children aged 0–14 years represent a disproportionately affected population, contributing substantially to the overall burden of disease and loss of productive life years [5]. The highest burdens have been reported in Asia and Africa, with countries such as Nepal, Myanmar, and Niger ranking among those most affected in 2019 [5].
Because rabies is predominantly transmitted through animal bites, several preventive measures have been implemented to reduce disease incidence. These include increasing public awareness, conducting mass dog vaccination programs to eliminate the disease at its source, providing pre-exposure prophylaxis (PEP) for individuals at increased occupational risk, such as veterinarians, and ensuring prompt PEP following animal bites or scratches. These interventions are consistent with the One Health approach, which recognizes the interconnectedness of human, animal, and environmental health and promotes multisectoral collaboration to prevent and control zoonotic diseases [7]. In support of this framework, the World Health Organization (WHO), World Organization for Animal Health (WOAH), and Food and Agriculture Organization of the United Nations (FAO) launched the United Against Rabies initiative to achieve the “Zero by 30” target, which aims to eliminate human deaths caused by dog-mediated rabies by 2030 [8, 9]. A key component of this strategy is the collection and integration of surveillance data through the Emergency Prevention System for Animal Health Information System Plus (EMPRES-i Plus), a publicly accessible platform that aggregates official reports of transboundary animal diseases, including rabies [10].
Despite substantial global efforts toward rabies elimination, important gaps remain in understanding the long-term spatiotemporal distribution of rabies events reported through integrated surveillance platforms. Most previous studies have focused on national or regional epidemiology, burden estimation, vaccination strategies, or modeling approaches, whereas comprehensive evaluations of global rabies reporting patterns using EMPRES-i Plus remain limited. Furthermore, few studies have examined the distribution of rabies reports across geographic regions, host categories, and reporting sources within a One Health surveillance framework. The coexistence of animal and human rabies records within EMPRES-i Plus provides a unique opportunity to explore the animal–human interface of rabies surveillance; however, this resource has been underutilized for global descriptive assessments. Consequently, there remains a need for a comprehensive analysis of worldwide rabies reporting patterns to identify regional variations, host-associated trends, and reporting characteristics that may inform future surveillance and control strategies.
Therefore, this study aimed to describe the global spatiotemporal patterns of confirmed rabies reports recorded in EMPRES-i Plus from 2014 to 2024. Specifically, the study evaluated the temporal distribution of reported rabies events, regional reporting patterns, host-category distributions, sources of report confirmation, and the geographic occurrence of human rabies cases within a One Health surveillance framework. By providing a decade-long overview of global rabies reporting, this study seeks to provide evidence to support the strengthening of integrated surveillance systems, improve cross-sectoral data utilization, and facilitate progress toward global rabies elimination goals. Surveillance performance, intervention effectiveness, and causal determinants of rabies incidence were beyond the scope of the present investigation.
MATERIALS AND METHODS
Ethical approval
This study used publicly available surveillance data from EMPRES-i Plus and therefore did not require review or approval by an institutional ethics committee [10]. The database is maintained and disseminated by FAO in accordance with its data-sharing, privacy, and citation policies. Human rabies records available in the database were reported in anonymized, non-identifiable form at the case level, and no personal identifiers were accessible to the investigators. Furthermore, the study did not involve direct interaction with human participants or animals, the collection of biological samples, or intervention procedures.
Study period and location
This study was conducted from August to October 2025 using confirmed rabies reports recorded in EMPRES-i Plus from January 1, 2014, to December 31, 2024. The study population comprised animal and human rabies reports submitted by reporting countries worldwide and available through the EMPRES-i Plus database.
Within EMPRES-i Plus, animal rabies is documented at the report level, whereas human rabies is recorded at the case level. Accordingly, animal rabies was analyzed using report-based records, whereas human rabies was analyzed using individual case records. Available variables included report identification number, reporting date, host species, host category (human, domestic animal, wild animal, or captive animal), locality, country, region, source of confirmation, and report status.
Study design and data collection
This study employed an observational, retrospective, descriptive surveillance design using secondary data obtained from EMPRES-i Plus, an open-access surveillance platform managed by FAO. The database aggregates animal disease reports from multiple official contributors and serves as a global repository for transboundary animal disease information. All data analyzed in this study were extracted exclusively from the EMPRES-i Plus interface. The investigation was descriptive and hypothesis-generating in nature and did not involve causal inference or inferential statistical modeling.
Data extraction was performed on August 8, 2025, using the EMPRES-i Plus web-based interface. Records were accessed through the Table panel and filtered using the following criteria: disease (“rabies”), diagnosis status (“all”), animal type (“all”), start observation date (January 1, 2014), and end observation date (December 31, 2024). No free-text keyword searches were performed. Only officially confirmed rabies reports recorded within the study period were included in the analysis. Suspected or unconfirmed records, reports outside the study period, withdrawn reports, duplicate entries identified during data processing, and records lacking essential variables required for classification were excluded when necessary.
EMPRES-i Plus reports officially confirmed rabies events submitted by national authorities; however, the database does not consistently differentiate laboratory-confirmed diagnoses from epidemiologically linked cases and does not systematically capture information on specific diagnostic methods, such as polymerase chain reaction or fluorescent antibody testing. Each record was treated as an independent reported event because unique outbreak-level identifiers are not consistently available across reporting countries. Host classification followed the standardized categories used within EMPRES-i Plus, including humans, domestic animals, wild animals, and captive animals, without further reclassification.
The EMPRES-i Plus database does not systematically record individual-level demographic information, such as age and sex, exposure pathways, or PEP data for human rabies cases. Consequently, stratified analyses based on these variables could not be performed. As a passive, event-based surveillance system, EMPRES-i Plus may also be affected by reporting bias, variability in national surveillance capacity, and differences in diagnostic confirmation practices across countries.
Data processing and analysis
The dataset was cleaned and organized using Microsoft Excel for Microsoft 365 (Microsoft Corporation, Redmond, WA, USA). Only officially confirmed rabies reports recorded during the study period were retained for analysis. EMPRES-i Plus was used solely as a data source and visualization platform; no analytical or statistical tools embedded within the database were used.
All numerical summaries were calculated offline using the exported dataset. Analyses were restricted to descriptive statistics, including frequencies and proportions, to summarize annual reporting trends, regional distributions, host-category distributions, sources of report confirmation, and the geographic distribution of reported human rabies cases. Inferential statistical analyses, confidence interval estimation, and formal trend modeling were not performed. Therefore, all temporal patterns presented in this study should be interpreted as descriptive observations rather than statistically validated trends. Because the analysis was based on complete enumeration of all confirmed rabies reports and human rabies cases available during the study period, rather than sampled data or population-based estimates, confidence intervals were not calculated.
Data presentation
The global spatial distribution map of rabies reports was generated directly using the built-in mapping function available within EMPRES-i Plus and reproduced without modification. Map projection, scale, and spatial resolution are predefined by the platform and cannot be modified by users.
Additional descriptive figures were generated in Microsoft Word (Microsoft Corporation, Redmond, WA, USA) from the cleaned dataset. These visualizations were used exclusively to present aggregated frequencies and proportions and did not involve additional spatial analyses or statistical modeling.
RESULTS
Regional distribution of confirmed rabies reports
Over the study period, a total of 1,510 confirmed rabies reports were recorded across four major regions (Figure 1). Asia contributed the highest number of reports (n = 1,056), followed by the Americas (n = 319), Europe (n = 91), and Africa (n = 44). These findings represent absolute counts of reports and were not adjusted for population size, surveillance capacity, or reporting intensity. Therefore, regional differences should be interpreted cautiously because they may reflect variations in surveillance and reporting systems rather than actual differences in rabies burden.
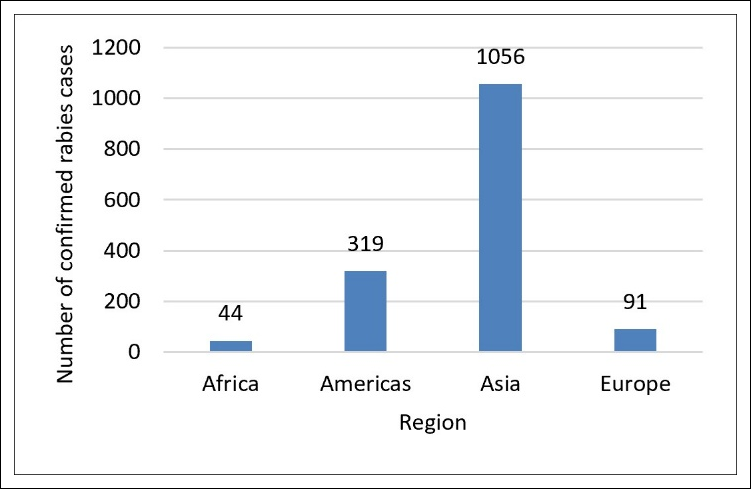
Figure 1. Regional distribution of confirmed rabies reports (2014–2024). Absolute numbers of reports by region.
Spatial distribution of confirmed rabies reports
The global spatial distribution of confirmed rabies reports is presented in Figure 2. Reported events were widely distributed across Africa, the Americas, Asia, and Europe. The map provides a descriptive overview of the geographic locations of reported rabies events generated directly from EMPRES-i Plus. No formal spatial clustering, hotspot analysis, or geospatial modeling was performed; therefore, the observed patterns should be interpreted qualitatively.
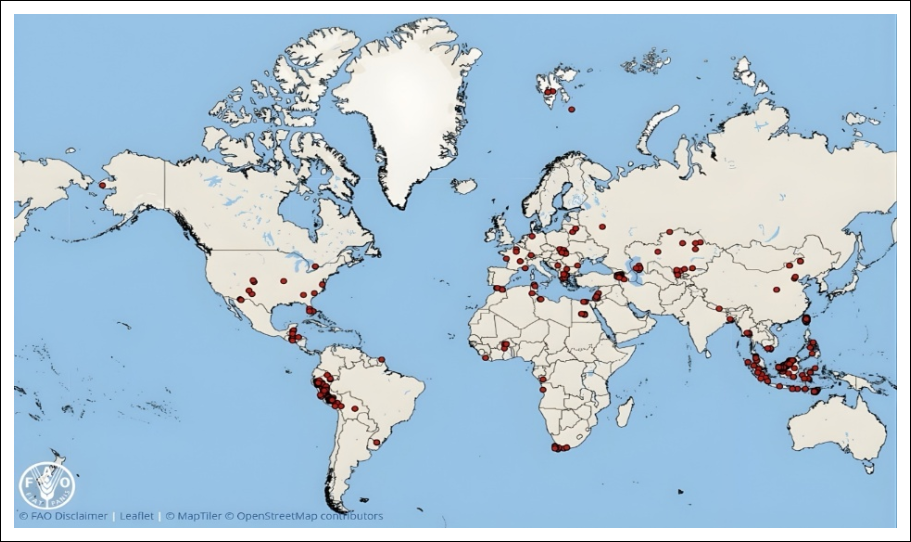
Figure 2. Global map of confirmed rabies reports, 2014–2024. Red markers indicate reported locations.
Temporal distribution of confirmed rabies reports
The annual number of confirmed rabies reports fluctuated considerably during the study period (2014–2024) (Figure 3). The highest annual number of reports was recorded in 2014 (n = 302), followed by secondary peaks in 2018 (n = 256) and 2019 (n = 233). In contrast, the fewest reports were observed in 2016 (n = 8). Overall, the data demonstrated substantial year-to-year variation without a consistent upward or downward trend over the study period. The unusually low number of reports recorded in 2016 may reflect reporting variability or incomplete data within EMPRES-i Plus, rather than a true decline in rabies occurrence. No stratified analyses based on policy implementation periods or the coronavirus disease 2019 pandemic were conducted.
Sources of rabies report confirmation
During 2014–2024, confirmed rabies reports originated from three principal reporting sources: WOAH, national authorities, and FAO field officers (Figure 4). Most reports were confirmed by WOAH, accounting for approximately 74% of all reports.
Within EMPRES-i Plus, reports attributed to WOAH may include notifications initially submitted by national authorities and subsequently validated through WOAH reporting mechanisms. Because the platform does not provide sufficient metadata to distinguish between overlapping submissions, reports were categorized by the primary confirmation source recorded in the database. Consequently, the predominance of WOAH-confirmed reports likely reflects the reporting hierarchy within the surveillance system rather than differences in surveillance activity among reporting sources.
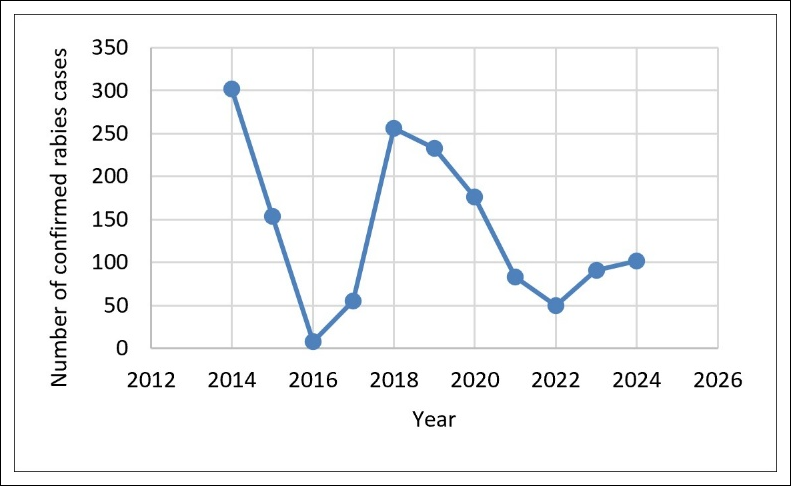
Figure 3. Temporal trend of confirmed rabies reports within the study period (2014–2024). A decline was observed from 2014 to 2016, followed by fluctuating annual reporting thereafter, with notable peaks in 2018 and 2019.
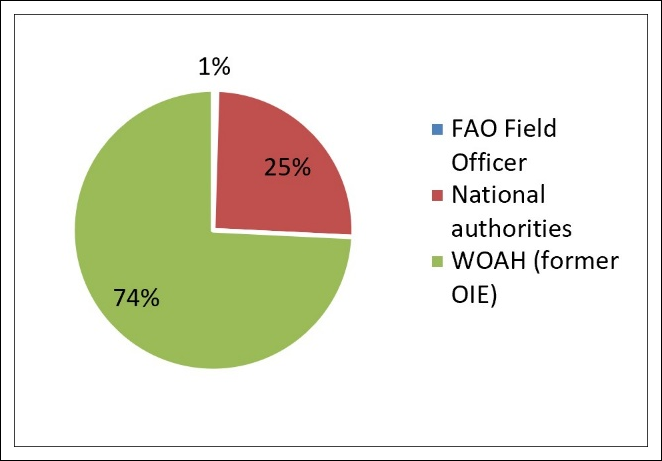
Figure 4. Proportion of confirmed rabies reports by source of confirmation. The majority of reports (74%) were confirmed through WOAH, followed by national authorities and FAO field officers.
Distribution of confirmed rabies reports by host-category and region
Confirmed rabies reports included both human and animal hosts across all four major regions (Table 1). Domestic animals constituted the predominant host category globally, accounting for 1,326 reports, followed by wild animals with 176 reports. This distribution pattern was generally consistent across regions. Captive animals were reported only twice and were recorded exclusively in Asia.
Host classification followed the EMPRES-i Plus reporting taxonomy, which categorizes reports into human, domestic animal, wild animal, and captive animal groups. Species-level information, including dog-specific records and wildlife species such as bats and foxes, was not consistently available across reports and therefore could not be analyzed reliably. Consequently, domestic animal reports were evaluated as an aggregated category rather than specifically as dog-mediated rabies. The captive animal category represented animals maintained under human management outside conventional domestic settings and contributed minimally to the overall dataset.
| Region | Human | Captive animal | Domestic animal | Wild animal | Total reports |
|---|---|---|---|---|---|
| Africa | 1 | 0 | 29 | 14 | 44 |
| Americas | 0 | 0 | 310 | 9 | 319 |
| Asia | 5 | 2 | 942 | 107 | 1,056 |
| Europe | 0 | 0 | 45 | 46 | 91 |
| Total | 6 | 2 | 1,326 | 176 | 1,510 |
Table 1. Distribution of confirmed rabies reports by host-category and region, 2014–2024.
| Region | Human | Captive animal | Domestic animal | Wild animal | Total reports |
|---|---|---|---|---|---|
| Africa | 1 | 0 | 29 | 14 | 44 |
| Americas | 0 | 0 | 310 | 9 | 319 |
| Asia | 5 | 2 | 942 | 107 | 1,056 |
| Europe | 0 | 0 | 45 | 46 | 91 |
| Total | 6 | 2 | 1,326 | 176 | 1,510 |
Geographical distribution of human rabies cases
A total of 27 human rabies cases were recorded in EMPRES-i Plus during the study period, resulting in 20 reported deaths. This corresponded to an overall case fatality rate of approximately 74.1%. All reported fatalities occurred in Africa and Asia.
Individual-level demographic characteristics, including age and sex, as well as exposure pathways and PEP status, were not systematically available within EMPRES-i Plus. Consequently, detailed demographic analyses could not be performed. The reported human rabies cases should therefore be interpreted as surveillance records captured within an animal-centered reporting system rather than as comprehensive descriptions of the global human rabies burden.
| Locality | Country | Region | Report date | Humans affected | Human deaths |
|---|---|---|---|---|---|
| Luanda | Angola | Africa | 24/02/2015 | 18 | 18 |
| Serian | Malaysia | Asia | 12/07/2017 | 4 | 2 |
| Phu Tuc commune, Chau Thanh district | Vietnam | Asia | 23/05/2022 | 1 | 0 |
| Hoa Nghia commune, Cho Lach district | Vietnam | Asia | 23/05/2022 | 1 | 0 |
| Mo Cay town, Mo Cay Nam district | Vietnam | Asia | 23/05/2022 | 2 | 0 |
| An Hoi ward, Ben Tre district | Vietnam | Asia | 23/05/2022 | 1 | 0 |
| Total | - | - | - | 27 | 20 |
Table 2. Reported human rabies cases recorded in EMPRES-i Plus during 2014–2024
| Locality | Country | Region | Report date | Humans affected | Human deaths |
|---|---|---|---|---|---|
| Luanda | Angola | Africa | 24/02/2015 | 18 | 18 |
| Serian | Malaysia | Asia | 12/07/2017 | 4 | 2 |
| Phu Tuc commune, Chau Thanh district | Vietnam | Asia | 23/05/2022 | 1 | 0 |
| Hoa Nghia commune, Cho Lach district | Vietnam | Asia | 23/05/2022 | 1 | 0 |
| Mo Cay town, Mo Cay Nam district | Vietnam | Asia | 23/05/2022 | 2 | 0 |
| An Hoi ward, Ben Tre district | Vietnam | Asia | 23/05/2022 | 1 | 0 |
| Total | - | - | - | 27 | 20 |
Note EMPRES-i Plus = Emergency Prevention System for Animal Health Information System Plus.
DISCUSSION
Temporal patterns of rabies reporting
Rabies is considered a neglected tropical disease, and many countries have not yet succeeded in eliminating it. To achieve the Zero by 30 goal, which aims for zero human deaths caused by dog-mediated rabies by 2030, multidisciplinary preventive measures and reliable surveillance data are essential.
One Health programs for vaccination and surveillance have been implemented in several rural communities and have successfully reduced human rabies incidence, highlighting the importance of integrated approaches endorsed within the global Zero by 30 strategy [11, 12]. Recent analyses have further demonstrated that regions implementing coordinated One Health strategies, such as Rwanda and the Philippines, experienced reductions in rabies transmission events, supporting the premise that interdisciplinary collaboration enhances disease control [13]. Mass canine vaccination programs in several endemic countries have reduced human rabies mortality by more than 80%, underscoring the pivotal role of coordinated One Health interventions [14]. Moreover, field-level evidence from Moshi, Tanzania, demonstrated that district-based One Health approaches can effectively address local cultural factors influencing rabies control. When combined with routine canine vaccination programs, these interventions can reduce the propagation of outbreaks and animal rabies cases [15]. In Indonesia, the One Health approach has also contributed to rabies control. A study conducted in Ketapang District, West Kalimantan, reported a reduction in disability-adjusted life years associated with rabies, indicating the effectiveness of integrated One Health interventions [16].
The temporal patterns observed in the present study may align with broader global efforts to strengthen rabies control under the Zero by 30 initiative, although causal relationships cannot be inferred due to the study's descriptive design. This interpretation is supported by reports from several countries. For example, implementation of the Stepwise Approach Towards Rabies Elimination (SARE) tool and integration of One Health principles into national rabies control programs in Ethiopia have been associated with improved vaccination coverage and surveillance reporting [17]. However, challenges remain. A study conducted in Indonesia reported that the One Health approach for rabies prevention and control in West Kalimantan was difficult to sustain without continuous training of animal health personnel [18]. Other studies have similarly demonstrated that cultural beliefs, inadequate awareness, and delays in seeking appropriate medical care after animal bites continue to hinder rabies control efforts. In some settings, individuals preferentially seek traditional healers rather than healthcare facilities after dog bites, underscoring the importance of multisectoral approaches that engage local community leaders and other stakeholders [11, 17].
In the present time series, reporting increased after 2022. Although the dataset's descriptive nature does not permit causal attribution, this pattern may reflect disruptions to rabies surveillance and control activities during the coronavirus disease 2019 pandemic in the preceding years. This interpretation is supported by reports from several countries in the Americas that documented increases in rabies cases following the pandemic period [19]. Future rabies control efforts should therefore address potential setbacks associated with the pandemic while maintaining mass canine vaccination programs in low- and middle-income countries, strengthening systematic wildlife surveillance in regions with predominant wildlife reservoirs, and promoting broader ecosystem-based One Health frameworks. Investment in real-time cross-sectoral data integration is also necessary to facilitate early outbreak detection and improve monitoring and evaluation of One Health interventions. Persistent gaps in cross-sectoral data sharing and limited resources in low-income settings remain barriers to achieving the Zero by 30 targets, highlighting the need for strengthened One Health governance and sustained financial investment [20]. Furthermore, incorporation of wildlife reservoirs and ecological risk mapping into One Health initiatives may facilitate a more comprehensive and holistic framework for rabies control [7, 21].
Regional and host-associated patterns of rabies reporting
The regional analysis of the EMPRES-i Plus dataset demonstrated that domestic animal reports predominated in Asia and the Americas, whereas wildlife-associated reports represented a larger proportion of records in Europe and Africa. These findings should be interpreted cautiously because surveillance intensity, reporting infrastructure, diagnostic capacity, and animal population density may substantially influence observed reporting patterns. The regional differences observed in the present study may also reflect surveillance visibility bias. Regions with established canine vaccination and rabies control programs, particularly in Europe and the Americas, may report relatively greater numbers of wildlife-associated cases because wildlife surveillance systems become more prominent following successful reductions in dog-mediated rabies [22]. Conversely, regions with weaker surveillance systems may experience a substantial but largely undocumented rabies burden because many cases remain outside formal reporting structures [22]. Recognition of these factors is essential when interpreting event-based surveillance databases such as EMPRES-i Plus.
In the Americas, the Pan American Health Organization has coordinated the Regional Program for the Elimination of Dog-Mediated Human Rabies since 1983, achieving reductions exceeding 95% in canine-transmitted human rabies cases through mass dog vaccination and expanded access to PEP [23, 24]. Similarly, the Animal and Plant Health Inspection Service of the United States Department of Agriculture has implemented national wildlife rabies management programs targeting raccoons, skunks, foxes, and bats through oral vaccination bait strategies [25]. In Europe, rabies control efforts have increasingly focused on wildlife reservoirs through oral rabies vaccination programs supported by the European Commission. These programs have successfully eliminated fox-mediated rabies from most Western and Central European countries through aerial distribution of vaccine baits [26, 27].
In contrast, higher densities of free-roaming dogs and variable surveillance capacities may contribute to the predominance of reports of domestic animal-associated cases in Asia and Africa [28]. Regional rabies control networks, including the Pan-African Rabies Control Network and the Middle East, Eastern Europe, Central Asia, and North Africa Rabies Control Network, were established to support rabies elimination efforts in endemic countries. These initiatives utilize tools such as SARE to facilitate the transition from endemic rabies to zero human deaths and are frequently supported by the Global Alliance for Rabies Control and the Zero by 30 Global Strategic Plan [29, 30]. These coordinated programs emphasize large-scale dog vaccination and community-based surveillance to bridge the gap between resource-limited settings and global rabies elimination targets [31, 32]. Therefore, the regional patterns observed in the present study likely reflect both underlying epidemiological conditions and differences in surveillance capacity, highlighting the importance of integrated animal surveillance systems within region-specific rabies control frameworks.
Human rabies cases within a One Health surveillance framework
High vaccine costs, inadequate surveillance infrastructure, limited intersectoral collaboration, and insufficient public awareness remain major obstacles to rabies control worldwide [19, 21]. Inadequate prevention measures and poor post-exposure management continue to result in human rabies deaths, particularly in countries facing financial constraints and competing public health priorities.
EMPRES-i Plus recorded 20 human rabies deaths during 2014–2024. These deaths should be interpreted as sentinel indicators of failures in upstream prevention rather than as comprehensive estimates of the global human rabies burden. The number of deaths identified in EMPRES-i Plus is substantially lower than estimates reported by WHO and GBD. WHO reported 1,141 human rabies deaths globally in 2021, with 46.1% of these deaths occurring in the Western Pacific Region (n = 527). GBD estimated approximately 10,100 human rabies deaths during the same year [5]. The discrepancy between EMPRES-i Plus and WHO estimates may be explained by differences in surveillance objectives and data sources. During the study period, EMPRES-i Plus primarily compiled reports from WOAH, national authorities, and FAO field officers, and was designed primarily for animal disease surveillance rather than for comprehensive human disease surveillance. Human rabies cases reported within EMPRES-i Plus generally represented events that could be linked to animal outbreaks, whereas WHO datasets may include human cases that cannot be directly traced to specific animal sources. Furthermore, GBD estimates are derived from multiple sources, including surveillance databases, systematic reviews, and additional epidemiological datasets [5].
The coexistence of report-level animal data and case-level human data within EMPRES-i Plus illustrates a broader methodological challenge in the integration of One Health surveillance. Consequently, the human rabies cases identified in the present study may not fully represent the global burden of human rabies, as cases in remote or under-resourced regions may remain undetected or unreported.
Through its integration of animal and human health information, EMPRES-i Plus provides a unique opportunity to evaluate failures occurring at the animal–human interface. Unlike burden-estimation studies that focus primarily on total mortality, EMPRES-i Plus documents actual disease events occurring across animal and human populations. This capability enables identification of host-specific and regional variations, including the predominance of domestic animal-associated reports in Asia and the higher proportion of wildlife-associated reports observed in Europe. Because the platform prioritizes reports originating from animal health authorities and WOAH, human rabies entries can be interpreted as sentinel indicators of upstream prevention failures, including deficiencies in canine vaccination programs and wildlife rabies management. Consequently, EMPRES-i Plus provides a distinctive One Health perspective by documenting the operational interface of zoonotic transmission rather than solely estimating disease burden.
This concept is illustrated by the 2015 Luanda outbreak, which accounted for approximately 90% (n = 18) of human rabies deaths reported in EMPRES-i Plus during the study period. Although local epidemiological information remains limited, the Luanda outbreak may serve as an example of a breakdown in One Health prevention systems. Approximately 92% of fatalities reported between January and March occurred among children younger than 10 years of age, highlighting the severe consequences of inadequate rabies control measures. In response to the outbreak, Angolan authorities initiated a multisectoral campaign involving vaccination of dogs, cats, and monkeys. During the same period, WHO reported 151 human rabies deaths in Angola and 2,792 deaths globally. These observations further demonstrate the consequences of inadequate surveillance and fragmented control programs, and reinforce the need for robust One Health frameworks that integrate multiple sectors to prevent and control zoonotic diseases [33]. Reframing human rabies cases reported in EMPRES-i Plus as sentinel indicators of prevention failures underscores the importance of strengthening the animal–human surveillance interface to prevent spillover events and subsequent human deaths.
Policy implications for One Health surveillance
From a policy perspective, the findings of this study highlight the importance of strengthening harmonized surveillance frameworks across animal and human health sectors within a One Health governance structure. The relatively low number of human rabies cases captured within EMPRES-i Plus, which is primarily an animal-centered, event-based surveillance platform, underscores the need for improved cross-sectoral integration with human health surveillance systems, such as those maintained by WHO. Reducing reporting variability and enhancing global comparability of rabies surveillance data require standardized reporting procedures, interoperable metadata structures, and consistent data submission by national authorities. Strengthening surveillance systems in low- and middle-income countries, particularly in regions with high numbers of domestic animal-associated reports, may facilitate earlier detection and reporting of zoonotic transmission events.
Conceptually, rabies control within a One Health framework may be viewed as a Surveillance–Response–Outcome cycle. Event-based platforms such as EMPRES-i Plus provide the surveillance component by documenting rabies events and potential zoonotic transmission interfaces. These observations should trigger appropriate public health responses, including mass vaccination programs and access to PEP. Human rabies deaths may subsequently function as outcome indicators reflecting the effectiveness of prevention measures. Furthermore, improved alignment among FAO, WOAH, and WHO surveillance systems through integrated reporting pathways could support more accurate monitoring of progress toward the Zero by 30 rabies elimination targets.
Strengths and limitations
This study has several strengths. First, it utilized EMPRES-i Plus, a widely recognized FAO surveillance platform that compiles standardized animal health reports from WOAH, national authorities, and partner organizations, thereby enabling broad geographic coverage and facilitating cross-regional comparisons. Second, the 10-year study period (2014–2024) reduced the influence of short-term fluctuations in surveillance data and allowed evaluation of long-term reporting patterns. Third, by focusing on animal rabies reports and using WHO data as contextual information rather than formally integrating multiple databases, the analysis remained consistent with the structure and intended use of the EMPRES-i Plus platform. Additionally, rigorous data verification procedures, including manual review and spreadsheet-based cross-checking with temporal filtering, were implemented to ensure record consistency throughout the study period. However, because the analysis relied exclusively on EMPRES-i Plus without formal multi-database harmonization, the findings primarily reflect reporting patterns and surveillance capacity rather than actual epidemiological burden.
This study also has several methodological limitations. First, although EMPRES-i Plus aggregates animal health reports from multiple sources, including WOAH, national authorities, and FAO field officers, the analysis did not incorporate complementary human health surveillance datasets such as WHO databases [34]. Consequently, a comprehensive evaluation of global rabies trends across animal and human populations was not possible. Second, despite the use of standardized reporting procedures within EMPRES-i Plus, heterogeneity may still arise from differences in national reporting practices, diagnostic capabilities, and reporting formats [35]. Third, the patterns observed in this study likely reflect reporting practices, surveillance capacity, and submission behaviors, as well as underlying epidemiological conditions, particularly in regions with variable surveillance infrastructure. Therefore, these limitations should be interpreted as constraints of the study design and data source rather than inherent weaknesses of the EMPRES-i Plus platform itself.
CONCLUSION
This study provides a comprehensive overview of global rabies reporting patterns recorded in EMPRES-i Plus between 2014 and 2024 from a One Health perspective. A total of 1,510 confirmed rabies reports were identified, with Asia accounting for the highest number, followed by the Americas, Europe, and Africa. Domestic animals represented the predominant host category, whereas wildlife-associated reports were more prominent in certain regions. Temporal analysis demonstrated substantial year-to-year fluctuations in reporting, with the highest number of reports recorded in 2014 and additional peaks observed in 2018 and 2019. Human rabies cases captured within EMPRES-i Plus were limited, comprising 27 reported cases and 20 associated deaths, all occurring in Africa and Asia.
The findings highlight the continuing importance of integrated rabies surveillance systems for monitoring disease occurrence at the animal–human interface. The predominance of reports on domestic animal-associated cases reinforces the critical role of sustained canine vaccination programs, whereas regional differences in host categories emphasize the need for surveillance strategies tailored to local epidemiological conditions. The study further demonstrates the value of EMPRES-i Plus as a One Health surveillance platform capable of identifying temporal, regional, and host-associated reporting patterns that may support rabies prevention and control efforts.
A major strength of this study is the use of a globally accessible surveillance platform that compiles standardized reports from multiple official sources across a 10-year period, enabling broad geographic coverage and cross-regional comparisons. However, several limitations should be considered. The analysis relied exclusively on EMPRES-i Plus and did not incorporate complementary human health surveillance databases. In addition, variations in national surveillance capacity, reporting practices, and diagnostic confirmation may have influenced reporting patterns. Consequently, the observed trends should be interpreted as surveillance-based reporting patterns rather than direct measures of the true epidemiological burden of rabies.
Future studies should focus on harmonizing animal and human health surveillance databases, improving metadata completeness, and incorporating advanced analytical approaches, including spatial analyses, predictive modeling, and machine learning-assisted surveillance systems. Enhanced integration among FAO, WOAH, WHO, and national surveillance networks would strengthen global rabies monitoring and facilitate more accurate assessment of progress toward elimination targets.
Overall, the present findings underscore the need for strengthened One Health surveillance, improved cross-sectoral data integration, and sustained investment in rabies prevention and control programs. Such efforts will be essential for supporting evidence-based decision-making and accelerating progress toward the global Zero by 30 goal of eliminating human deaths caused by dog-mediated rabies.
DATA AVAILABILITY
The supplementary data can be made available from the corresponding author upon request.
GENERATIVE AI DECLARATION
The authors declare that generative artificial intelligence (AI) tools were used solely to improve language, grammar, and readability during manuscript preparation. All scientific content, data analysis, interpretation of results, and conclusions were developed and verified by the authors. The authors take full responsibility for the accuracy, integrity, and originality of the work presented, and no AI tool was listed as an author.
AUTHORS’ CONTRIBUTIONS
AAH and WKS: Conceptualization, data analysis, interpretation of results, manuscript preparation, and critical revision of the manuscript. DI: Data collection, data processing, initial data analysis, and manuscript preparation. All authors have read and approved the final version of the manuscript.
COMPETING INTERESTS
The authors declare that they have no competing interests.
PUBLISHER’S NOTE
Veterinary World remains neutral with regard to jurisdictional claims in the published institutional affiliations.
ACKNOWLEDGMENTS
The authors acknowledge the Faculty of Medicine and Nutrition, IPB University. The publication of this article was supported by the Directorate General of Research Enhancement and Development under the Publication Assistance Program, as stipulated in the Decree of the Director General of Research and Development No. 279/C/C2/KPT/2025 dated December 11, 2025.
REFERENCES
- Ashwini MA, Pattanaik A, Mani RS. Recent updates on laboratory diagnosis of rabies. Indian J Med Res 2024;159(1):48-61. [Google Scholar]
- Lojkić I, Šimić I, Bedeković T, Krešić N. Current status of rabies and its eradication in Eastern and Southeastern Europe. Pathogens 2021;10(6):742. [Google Scholar]
- de Lima JS, Mori E, Kmetiuk LB, Biondo LM, Brandão PE, Biondo AW. Cat rabies in Brazil: a growing One Health concern. Front Public Health 2023;11:1210203. [Google Scholar]
- World Health Organization. WHO fact sheets: Rabies [Internet] 2024. [Google Scholar]
- Gan H, Hou X, Wang Y, Xu G, Huang Z, Zhang T. Global burden of rabies in 204 countries and territories, from 1990;126:136-44. [Google Scholar]
- Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis 2015;9(4):e0003709. [Google Scholar]
- Acharya KP, Chand R, Huettmann F, Ghimire TR. Rabies elimination: Is it feasible without considering wildlife? J Trop Med 2022;2022:1-6. [Google Scholar]
- World Health Organization. Zero by 30: the global strategic plan to end human deaths from dog-mediated rabies by 2030. [Google Scholar]
- Tidman R, Thumbi S, Wallace R, de Balogh K, Iwar V, Dieuzy-Labaye I. United Against Rabies Forum: the One Health concept at work. Front Public Health 2022;10:854419. [Google Scholar]
- FAO EMPRES-i+. Global Animal Disease Information System [Internet]. Food and Agriculture Organization. [cited 2025. [Google Scholar]
- Fahrion AS, Freuling CM, Léchenne M, Müller T, Recuenco S, Vigilato MAN. Editorial: Rabies, a long-standing One Health example – progress, challenges, lessons and visions on the way to 0 by 30. Front Vet Sci 2023;10:1220327. [Google Scholar]
- Masthi NRR, Narayana DHA, Kulkarni P, Belludi A. Epidemiology and prevention of animal bite and human rabies in a rural community-One health experiment. Asian Pac J Trop Dis 2014;4:S486-90. [Google Scholar]
- Ahmed MM, Okesanya OJ, Othman ZK, Ibrahim AM, Adigun OA, Ukoaka BM. Holistic approaches to zoonoses: integrating public health, policy, and One Health in a dynamic global context. Zoonotic Dis 2025;5(1):5. [Google Scholar]
- Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet 2014;384(9951):1389-99. [Google Scholar]
- Mtui-Malamsha N, Sallu R, Mahiti GR, Mohamed H, OleNeselle M, Rubegwa B. Ecological and epidemiological findings associated with zoonotic rabies outbreaks and control in Moshi, Tanzania, 2017;16(16):2816. [Google Scholar]
- Aptriana CD, Sudarnika E, Basri C, Indrawan D, Daryono J, Suseno PP. Assessment of the burden of rabies in One Health approach control program in Ketapang District Indonesia: using zDALY. Prev Med Rep 2024;45:102838. [Google Scholar]
- Erkyihun GA, Deressa SG, Wakene WZ, Gari FR. Efforts of rabies elimination with a One Health approach and SARE tools in Ethiopia. Decod Infect Transm 2024;2:100028. [Google Scholar]
- Aptriana CD, Sudarnika E, Basri C. Nationally and locally-initiated One Health approach in controlling rabies in West Kalimantan, Indonesia. Vet World 2022. [Google Scholar]
- Rupprecht CE, Mshelbwala PP, Reeves RG, Kuzmin IV. Rabies in a postpandemic world: resilient reservoirs, redoubtable riposte, recurrent roadblocks, and resolute recidivism. Anim Dis 2023;3(1):15. [Google Scholar]
- Savadogo M, Zangré H, Nana SD, Ilboudo AK, Dahourou LD, Ilboudo SG. Adoption of the One Health approach to improve zoonosis control in low-income countries: insights from the case of rabies management in Burkina Faso. Int J One Health 2021. [Google Scholar]
- Ghai S, Hemachudha T. Continued failure of rabies elimination—consideration of challenges in applying the One Health approach. Front Vet Sci 2022;9:847659. [Google Scholar]
- Akinsulie OC, Adebowale OO, Adesola RO, Banwo OG, Idris I, Ogunleye SC. Holistic application of the One Health approach in the prevention and control of rabies: plausible steps towards achieving the 2030;6(1):22. [Google Scholar]
- Schneider MC, Belotto A, Adé MP, Hendrickx S, Leanes LF, Rodrigues MJ de F. Current status of human rabies transmitted by dogs in Latin America. Cad Saude Publica 2007;23(9):2049-63. [Google Scholar]
- Pan American Health Organization. World Rabies Day [Internet] 2024. [Google Scholar]
- US Department of Agriculture. U.S. National Plan for Wildlife Rabies Management 2023. [Google Scholar]
- Müller TF, Schröder R, Wysocki P, Mettenleiter TC, Freuling CM. Spatiotemporal use of oral rabies vaccines in fox rabies elimination programmes in Europe. PLoS Negl Trop Dis 2015;9(8):e0003953. [Google Scholar]
- Freuling CM, Hampson K, Selhorst T, Schröder R, Meslin FX, Mettenleiter TC. The elimination of fox rabies from Europe: determinants of success and lessons for the future. Philos Trans R Soc B Biol Sci 2013;368(1623):20120142. [Google Scholar]
- Misapa MC, Bwalya EC, Moonga L, Zimba J, Kabwali ES, Silombe M. Rabies realities: navigating barriers to rabies control in rural Zambia—a case study of Manyinga and Mwansabombwe Districts. Trop Med Infect Dis 2024;9(7):161. [Google Scholar]
- Lembo T, Attlan M, Bourhy H, Cleaveland S, Costa P, de Balogh K. Renewed global partnerships and redesigned roadmaps for rabies prevention and control. Vet Med Int 2011;2011:1-18. [Google Scholar]
- Zero by 30: the global strategic plan to end human deaths from dog-mediated rabies by 2030. [Google Scholar]
- Dodet B, Adjogoua EV, Aguemon AR, Amadou OH, Atipo AL, Baba BA. Fighting rabies in Africa: the Africa Rabies Expert Bureau (AfroREB). Vaccine 2008;26(50):6295-8. [Google Scholar]
- Knobel DL, Cleaveland S, Coleman PG, Fèvre EM, Meltzer MI, Miranda MEG. Re-evaluating the burden of rabies in Africa and Asia. Bull World Health Organ 2005;83(5):360-8. [Google Scholar]
- Haselbeck AH, Rietmann S, Tadesse BT, Kling K, Kaschubat-Dieudonné ME, Marks F. Challenges to the fight against rabies—the landscape of policy and prevention strategies in Africa. Int J Environ Res Public Health 2021;18(4):1736. [Google Scholar]
- Keshavamurthy R, Boutelle C, Nakazawa Y, Joseph H, Joseph DW, Dilius P. Machine learning to improve the understanding of rabies epidemiology in low surveillance settings. Sci Rep 2024;14(1):25851. [Google Scholar]
- Shams F, Jokar M, Djalali E, Abdous A, Rahnama M, Rahmanian V. Incidence and prevalence of rabies virus infections in tested humans and animals in Asia: a systematic review and meta-analysis study. One Health 2025;20:101102. [Google Scholar]